|
Scientists have identified thousands of genetic disorders. Fortunately most are quite rare and many are non life-threatening or treatable. Some are apparent in childhood while others do not manifest themselves until adulthood.
The public is aware of certain inherited diseases due to their frequency, severity and widespread publicity. These include cystic fibrosis, muscular dystrophy, hemophilia, Down syndrome and sickle cell anemia.
But do you know which is the most common, genetic, life threatening disease?
Most people do not know the answer—articles or lists of inherited conditions often do not mention this ailment yet this disease affects more people than all of the above mentioned inherited diseases combined!
Most people have never heard of this genetic disorder though it affects more than 600,000 Americans or about 1-in-400 adults—an estimated 12.5 million people worldwide regardless of sex, age, race or ethnic origin.
Upon hearing of this disease many think it is new. In fact, once often labeled Bright's disease in the 1700s and 1800s, we now know many cases were occurrences of this life threatening sickness.
This genetic disease has no cure and is technically designated "genetically autosomal dominant" meaning the chance of receiving the gene is 50%. (About 10% may come from sporadic mutations.) Either sex has an equal chance of receiving the gene and either parent can transmit the disease.
We now call this inherited disease:
Autosomal Dominant Polycystic Kidney Disease or ADPKD (or often PKD).
Note: A recessive, deadly form, Autosomal Recessive Polycystic Kidney Disease (ARPKD), is far less common, affecting mostly newborns, infants and children.
|
My maternal grandfather died of complications of PKD (renal failure) in his early 50s although no one knew the underlying cause.
Those afflicted with PKD may produce many cysts in the kidneys that fill with fluid and grow and multiply sometimes causing the kidneys to swell enormously from small dots to softball size. Ultimately, diseased kidneys may shut down. The result is end-stage renal disease and death. PKD has no known cure. The only forms of "treatment" are dialysis and transplantation.
Other organs may also grow cysts especially in the liver but these cysts typically do not cause organ failure. People with PKD may also experience urinary tract infections, blood in the urine, liver and pancreatic cysts, abnormal heart valves, high blood pressure, kidney stones, back and side pains and diverticulosis. Problems in other organs, such as the heart and blood vessels in the brain and leading to the brain, can cause aneurysms and death even in middle age.
PKD usually does not exhibit until one reaches early or middle adulthood. Some with PKD are fortunate and can lead normal lives with only minor problems. However, 50% of patients with PKD have kidney failure by age sixty.
My mother died at age sixty from complications due to PKD.
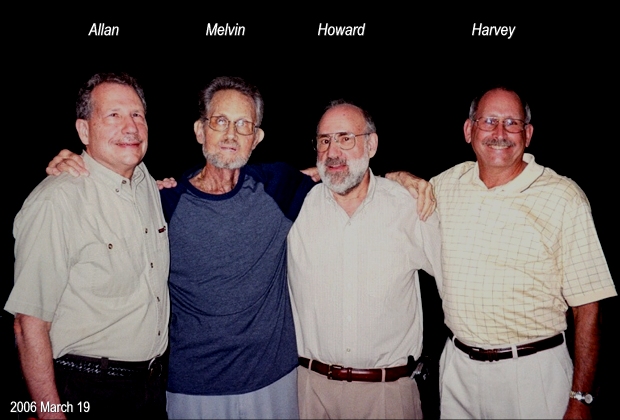
I have two younger brothers (Allan and Harvey, the youngest) plus a fraternal twin, Melvin, twelve minutes older. Statistically, because PKD is autosomal (non-sex) dominant, two of my parents' four children should have inherited PKD. Fortunately only one did.
My twin brother Melvin was the unfortunate one.
In his thirties, Melvin found he had high blood pressure. Subsequently, Melvin learned he had PKD. Kidney failure forced him to become a dialysis patient to survive. He was on home hemodialysis for eight years, three times per week for several hours each with his caring wife Linda attending. A complex dialysis machine removed large amounts of his blood from an access in his arm and returned this life giving fluid cleansed of waste products and excess liquids.
Although life savings, dialysis treatment takes its toll—fatigue, headaches, dietary worries, long term problems with access to blood vessels, infections, concern about a shortened life span, etc. His arms ultimately became strangely mutilated and scarred from constant use of the access ports in his limbs. Travel was difficult or impossible. Still, he managed to work, care for his family and was a loving father to his two daughters.
At age 47 I gave my twin a kidney. Although my fraternal twin and I were very different in both appearance and interests, we had an amazing six-antigen match, the best compatibility for people not identical twins. This kidney helped give Melvin a renewed life and freedom. He was now free from dialysis and even managed to make thirty-seven cruises with his wife over the next eighteen years!
Yet all was not well. Transplant patients do not always lead a life free of debilitating problems. A perforated duodenum from an endoscopic examination for a stress ulcer caused unending years of abdominal pains and cramping, diarrhea, and dietary distress (dumping syndrome). My brother developed a retinal detachment and became blind in his left eye. His right eye also experienced a retinal tear that was only partially repairable leaving him with poor vision.
(Continue on to next column)
|
My Twin (left) and I (right) — May 29, 2006 |
Effects from years of using antirejection drugs, especially prednisone, caused severe side effects including bruising of the skin leaving his skin "paper thin," delayed wound healing and increased risk of infection. He suffered through diarrhea, decreases in potassium blood levels, sodium and fluid retention with swelling in ankles, and loss of calcium from bone. Melvin was also severely lactose intolerant, which made replacing calcium difficult. Finally, endless skin and lip cancers due to prolonged use of prednisone, required partial removal of skin from his face, lips and ears.
Later Melvin also developed thyroid cancer and had this essential organ and part of his salivary glands removed. In addition, chemotherapy for a bout with colon cancer almost killed him due to his weakened immune system. He was also subject to infections since he needed to take immunosuppressive drugs to prevent kidney rejection. He developed osteoporosis and arthritis, and bled easily from tissue-thin skin. His feet and legs pained from fluids swelling his feet and legs. And his skin bore the puncture marks and scars of his years on dialysis, operations and medical treatment.
Finally, my brother could not walk. Between his dumping syndrome and diet problems, his weight dropped to less than 120 pounds though he had been a vigorous, six-foot tall man. Melvin often spent several days per week traveling to doctors futilely seeking help from his ailments and pains.
Appreciating the physical and mentally devastation caused by PKD on both my brother and his family for nearly thirty years is difficult if not impossible to explain, comprehend or visualize.
Nevertheless, Melvin persevered through his agony and tribulations for most of his adult life, including his eight years on dialysis and eighteen with his new kidney. I came to realize my twin was the bravest man I have ever known—a true hero and idol in the eyes of family and friends.
Finally, after eighteen years living with my still working kidney, Melvin's worn, diseased and distressed body failed.
I lost my twin brother at age sixty-six due to the dreadful consequences of PKD (2006 July 13).
So, why have so few heard of this often devastating disease?
Unknown for many years and often confused with other kidney disorders, no formal organization existed to take up the cause. Today, only one organization focuses on polycystic kidney disease, the PKD Foundation, not formed until the mid-1980s. Only now is PKD starting to gain some recognition and awareness. PKD also does not exhibit obvious external effects because the disease manifests itself on internal organs. PKD patients can have pain and wounded organs but otherwise may appear outwardly "normal." So, the disease goes unnoticed and persons with PKD will usually not attract attention or empathy from people who have no knowledge of this tragic disease.
Unfortunately, too, PKD has no well-known "celebrity" promoting its cause, and has not had any grand telethons to raise awareness and money. Indeed, many with PKD seem shy about promoting their illness. Consequently, few people know about PKD or can appreciate the untold agony this disease can cause on PKD patients and their families.
Interestingly, the eighteenth letter of the Hebrew alphabet, Chai ("living"), symbolizes life. Ironically, my Hebrew name is Chaim "life." And this too is the number of years my kidney gave my twin brother a new life though these years were not without ordeal.
You too can help those who live daily with this dreaded disease. You too can give hope to those yet to be born with PKD. Each fall, local chapters of the PKD Foundation now sponsor "Walks for PKD." In my hometown, Gainesville, Florida, the 2006 PKD walk was set for September 17.
However, I decided to participate in the 2006 PKD Walk in Palm Beach (Saturday, September 16) in order to join my two other brothers, Allan and Harvey, who live in South Florida.
(See Mel's Family and Friends below.)
Donations for PKD will help improve clinical treatment of Polycystic Kidney Disease, aid research to discover a cure, and make the more public aware of this potentially devastating, life threatening disease.
My brother has passed on but I am sure he would be grateful.
So will his family, friends and all victims of PKD.
¯¯¯¯¯¯¯¯¯
|



{kind=link}
{kind=link}